
By Adelaide Masterson
On President Trump’s first day back in office on January 20, 2025, he issued an executive order to withdraw the United States from the WHO and freeze all future transfers of US funding to the organization. Many have been pondering what this move means for our collective health in the US.
Modularity Theory suggests that the US is a key component in a deeply interdependent WHO. Pulling the US out could dismantle global health protection. Several months after the executive order, let’s take a peek and see what theory tells us is around the corner in both the near- and long-term.
An overview of Modularity Theory
A system’s architecture defines how its components and systems fit and function together to achieve a desired outcome. The theory refers to the areas where these parts come together as an interface. The components can be people, teams, or organizations, and the system’s architecture can be modular or interdependent at these interfaces.
If the interface is modular, it means that these components fit and function together in well-understood ways. The architecture of a modular system specifies this fit and function so well that anyone can make the components or subsystems, as long as these parts meet the required specifications. The components are designed to work independently as long as they conform to a standard interface. Modular interfaces are specifiable, verifiable, and predictable.
For example, I’m using a wireless keyboard and mouse to type this on my MacBook. I could’ve gotten an Apple keyboard and mouse, but I chose to get a Logitech one. I can select Logitech over Apple because both companies’ keyboard sets meet the exact specifications for my MacBook, they can easily verify that these specifications have been met, and there are no unpredictable interdependencies in the MacBook-keyboard interface. Therefore, this interface is modular.
If the architecture is interdependent at one of these interfaces, it means that one part can’t be created independently of the other. The two individual parts are tightly connected or woven together and likely rely on each other to function well. As a result, coordination within the system and among pieces is required for the system to function as intended. Therefore, the architecture must be integrated and tightly coordinated to deliver the necessary performance.
In the case of the WHO, member nations are the components that make up the global health organization’s interdependent architecture. The WHO is interdependent because each nation has its own set of priorities and challenges that also shift over time, meaning that international relations and how each country responds to disease outbreaks and contributes to the WHO are all fairly unpredictable interfaces.
What does the theory predict will happen?
Over the next five years, we can expect a steady stream of consequences resulting from the US’s withdrawal. The US supplies about one-fifth of the WHO’s $6.8 billion budget, in addition to a highly advanced network of health experts and considerable negotiating leadership. In the wake of this withdrawal, the WHO is experiencing a budget crisis unlike anything it has seen before. Smaller country contributions cannot fill the deficit, leaving the WHO to rely on budget cuts and diversification of its cash flow to mitigate this crisis. Due to its notable financial contributions, the US has always been a leader in WHO discussions and negotiations. Although these continue in the US’s absence, WHO members have noted a leadership vacuum since January 2025.
For these reasons, the WHO is likely to experience serious performance consequences within the next five years and potentially beyond. These consequences include: a significant drop in funding, faltering global health communication, and a lack of scientific expertise available to both the US and the WHO.
This isn’t my opinion. It’s an observation based on the predictive capability of Modularity Theory.
In the short term, reduced US funding will hinder the WHO’s efforts, leaving the US to face health emergencies alone and creating a gap in infrastructure and governance. We are already seeing this play out.
Funding: The WHO is funded through assessed contributions (a sliding scale of set amounts paid by each member nation) and voluntary contributions (funds typically allotted for specific projects). Of the WHO’s total revenue, assessed contributions account for approximately 12%, while voluntary contributions comprise about 87% (the remaining 0.6% is classified as “other”).
The US is the top member-nation contributor to the WHO (see figure below). For the past decade, its WHO donations have totaled $163 million to $816 million per year (the total fluctuates on an annual basis). The US contribution in 2022-2023 accounted for 16% of the WHO’s total revenue, totaling $1.28 billion. Only the Gates Foundation has surpassed this amount.
Contributions from other member nations are smaller and cannot compensate for the hole left by the US. As economic uncertainty becomes a larger global concern, many of these countries are unwilling or unable to increase their contributions.
Although the US can’t rescind funding or contributions pledged in advance, US funding has been paused for many voluntary programs, including the Global Polio Eradication Initiative (GPEI). Other significant voluntary contributions from the US strengthened access to essential health services, health emergency detection and response, epidemic and pandemic prevention, and global health emergency preparation. While the US is required to pay out any outstanding funds if it wishes to leave the WHO, the immediate freeze strained ongoing foreign aid efforts in the interim.
Therefore, American withdrawal will leave an enormous gap in the WHO budget, and there is no certain fix.
Top 25 contributors to the WHO from 2024-2025.
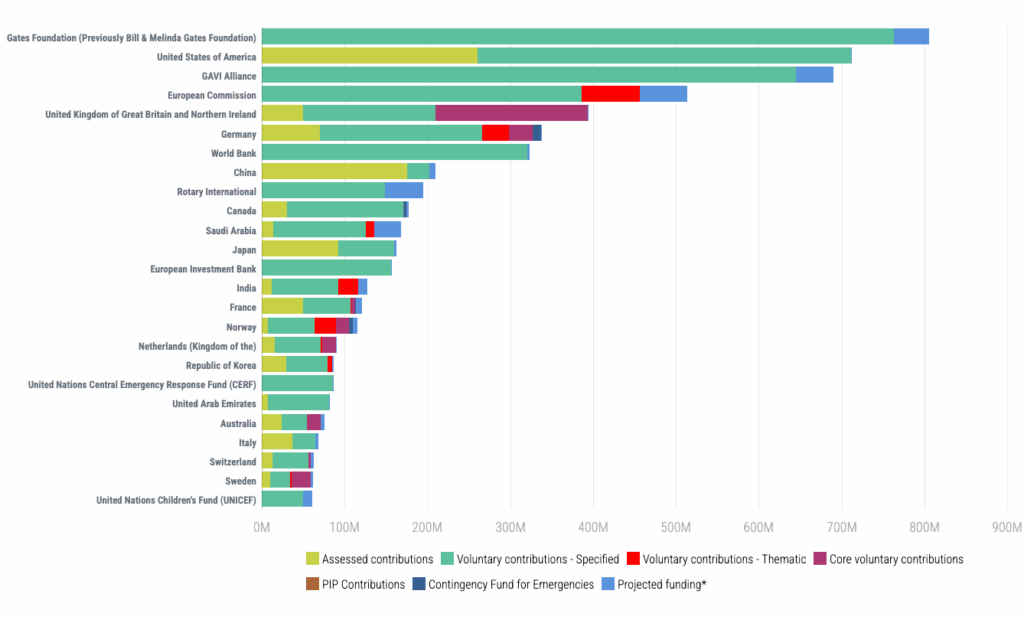
Source: https://open.who.int/2024-25/contributors/top25
Health emergencies: The US has also provided extensive technical support to the WHO. US government experts conduct research and laboratory work in collaboration with a network of WHO collaborating centers, including Johns Hopkins University, the Centers for Disease Control and Prevention (CDC), Boston University, and others. But all technical personnel working regularly with the WHO have been recalled, so this work has ceased. The WHO had also partnered with the US to handle international health emergencies and outbreaks. Now, the US will have to handle health crises, such as the recent avian influenza and measles outbreaks, on its own. That may or may not be an effective strategy, given the interdependent nature of global health.
Infrastructure: The US and its institutions were also vital supporters of the WHO’s efforts to build the global health workforce and strengthen regulatory systems worldwide. America has developed digital health systems and budget management processes, and it has shared its expertise with the WHO through various collaborating centers based in the US.
The Trump administration has also halted all communications between the CDC and the WHO. This communication has been crucial to supporting infectious disease response in low- and middle-income countries. The surveillance, contact tracing, and public health communication capacity of the US has helped address outbreaks of mpox (previously known as monkeypox), Marburg virus disease (MVD), and Ebola. Without American support, the global response, coordinated by the WHO, would have likely been less effective. In the interdependent structure of the WHO, the US is one component that has served as an active and vocal benefactor, often in unparalleled ways.
Governance: The American government has also been a core participant in WHO governance; however, our government will no longer have influence over what is prioritized within the WHO. The US was a leader in the Global Polio Eradication Initiative (GPEI). Without US financial support and CDC expertise and operational leadership, GPEI likely wouldn’t have seen such an extreme reduction in global polio cases. The US played a pivotal role in the pursuit and reduction of polio globally. Polio eradication was a US national interest and received bipartisan support for many years. Because of its considerable leadership and negotiating power, the US was able to pursue this goal with the support of the WHO.
These short-term impacts matter in and of themselves, but they also have downstream consequences that lead to long-term results—many of which are unappealing for public health.
In the long term, global health will falter, and funding cuts will lead to increased disease prevalence, higher health care costs, and reduced disease surveillance and communication.
Funding backfill: An investment round was opened to raise donations to fill the gap from the US withdrawal, but it’s unclear where that funding will come from. Although not as drastic as the US, contributions from other member nations have also been cut. As a result, the WHO is estimated to have lost about 17% of its funding within the last year. That amount is forecasted to decline further in the coming years, with no signs of recovery until 2030 or beyond. The most recent budget proposal for the next two years has decreased by 22% from the original plan. Without this money, much of the WHO’s work will struggle to continue.
Following this withdrawal, the Gates Foundation is now the WHO’s most significant benefactor. Unfortunately, in twenty years, the foundation will close its doors. Twenty years is a considerable amount of time for the WHO to develop a financing plan, but we may be seeing these consequences all over again if the US never rejoins the WHO.
Lack of expertise: Even if the money came from other sources, both the US and the WHO would be left without significant scientific expertise in the long run, which would hinder health and disease management globally. Eliminating its communication at prior interfaces—the connections between WHO member nations—means the US will be less prepared for emerging health threats, and the WHO will be left without a key member to contribute to ongoing studies.
Higher health care costs and disease risk: While this move will save the US money in the short term, the resulting health care burden will increase. As US investment in health preparedness dwindles, the American people are likely to experience a rise in the prevalence of infectious and communicable diseases. After all, infectious diseases know no borders (as COVID-19 so clearly taught us). Additionally, the US withdrawal will seriously hinder global disease response capacity. By removing ourselves from the WHO, both the US and the WHO are left with diminished capacity for surveillance, communication, and treatment research and development. As a result, diseases will spread more freely and become more prevalent worldwide.
Additional withdrawals: The withdrawal may also lead other member nations, such as Argentina, to withdraw from the WHO, which could exacerbate the effects of the US withdrawal. Losing its vast network of member nations may result in further desperate investment calls from the WHO and diminish the established credibility of the organization as a whole.
Modularity Theory predicts not just the impact on the WHO, but also on other global health initiatives
The immediate and predicted long-term impacts of this withdrawal underscore the interdependent and highly integrated nature of the WHO’s architecture. Theory says that removing or altering a key component (by cutting funding or withdrawing support) can lead to cascading failures and disarray, a scenario we’re already witnessing with US funding and communication cuts. Like other interdependent architectures, the WHO is reliant on each member nation’s support to function as intended. Withdrawing the US has the potential to impact the entire system’s performance and stability.
However, the WHO operates within the broader United Nations system, which is part of the global health landscape—an interdependent system within an interdependent system, within an interdependent system. Disease spreads without boundaries. A global, organized response is necessary to reduce mortality and morbidity worldwide. Losing one of the largest health care partners will be a loss felt by the American people, members of the WHO, and populations worldwide.
The challenges associated with this loss are significant, but they also present a unique opportunity to transform the frameworks that comprise global health as we know it. We could create an international health infrastructure that is more resilient and adaptable than ever before. One that doesn’t rely on the whims of a single administration or political polarization. One that not only survives a superpower’s withdrawal, but adapts and becomes modular because of it.