
Devin Bean, a research assistant at the Clayton Christensen Institute, and I coauthored this piece.
One thing the health care industry should admire about Wall Street capitalists is their ability to define their target and measure how well they are doing in achieving their aim. Most people would agree the aim of capitalism is profit (saying nothing of whether that is the right aim or not). The measures of that aim are reasonably straightforward using a standardized language of accounting rules. These standardized rules make it easy to compare one business to another using financial ratios (e.g., profit margin, return on capital, return on assets, etc.). When armed with knowledge of the rules and data to compute the financial ratios, deciding what to invest in becomes fairly straightforward—you invest in the opportunities that drive the highest profits over the shortest period of time.
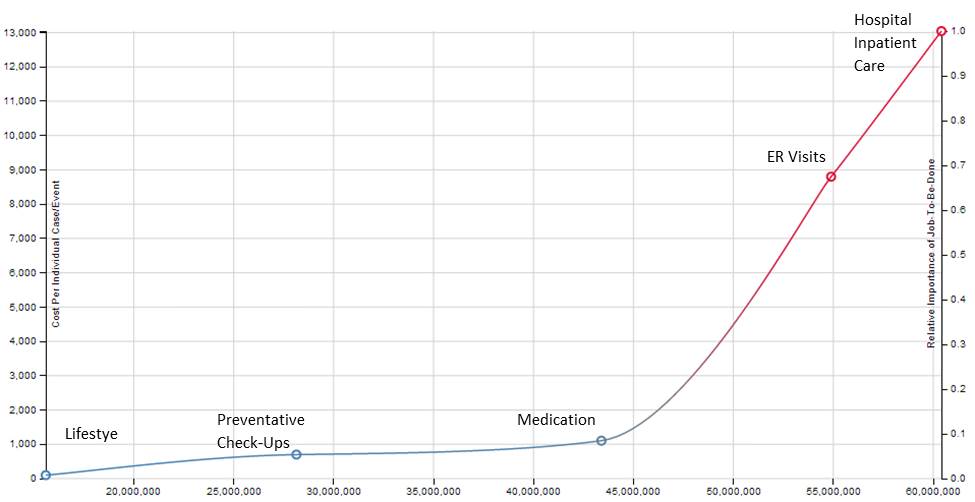
What is the aim of health care? Many of us would say it is health. If that is the case, however, we have been rotten resource allocators. Take diabetes, for example. In 2011 there were over 60 million care events in the U.S. related to diabetes. The cost per episode is plotted on the chart below. It clearly shows (not surprisingly) that the sicker you get, the more expensive your care is. This is not to say that we shouldn’t spend anything on very sick patients. What it does indicate is that though we say we value health, we actually choose to spend our money on sickness.
Source: Data compiled from Centers for Disease Control and Prevention/National Center for Health Statistics reports, including “National Diabetes Fact Sheet 2011,” “Self-report of Diabetes and Claims-based Identification of Diabetes Among Medicare Beneficiaries,” “National Ambulatory Medicare Survey,” “Summary Health Statistics for Adults.”
What would need to change to aim the health care system at health (vs. sickness) and effectively measure our returns on that investment? Here are a few thoughts:
1) Institute a common language for measuring health (and return on health investment)—Countries with developed capital markets almost always have a regulator that imposes a standardized language for financial measurement and reporting. In the United States this regulator is the Securities and Exchange Commission and the standardized language is Generally Accepted Accounting Principles (GAAP). Professor Regina Herzlinger of Harvard Business School has advocated for an ‘SEC’ for healthcare measurement and reporting. We join her chorus in advocating for this as a critical foundational need on which to base improvement going forward.
2) Create business models that make money on health (instead of sickness)— Patients have jobs to be done related to both health and sickness. Unfortunately, in the United States, providers by and large can only be paid for treating sickness, so the incentive to create businesses truly focused on health has been low. That is changing with the advent of new payment models and technologies such as telehealth, remote monitoring, and predictive analytics. We encourage entrepreneurs to ambitiously pursue business models where providers can make money on health care independent of sick care.
3) Drive care to lower acuity settings—As we can see from the diabetes graph above, spending per care event is much lower when those events occur in lower acuity settings. We hope patient and payor confidence in the quality of care delivered for precision medicine conditions will continue to grow and that more and more volume of care will shift to lower acuity settings.
We are optimistic that the next generation will grow up in a world where they will be able to evaluate and invest in return on health investment in the same way we look at margin or return on capital today. We applaud the innovators and entrepreneurs that are laying the groundwork for that future now.