
Loneliness is killing us. The Surgeon General’s advisory on our loneliness epidemic includes the chart shown below. It highlights the fact that lacking social connection is the new smoking. About a decade ago, sitting was the new smoking. But lacking social connection, it seems, may be even worse.

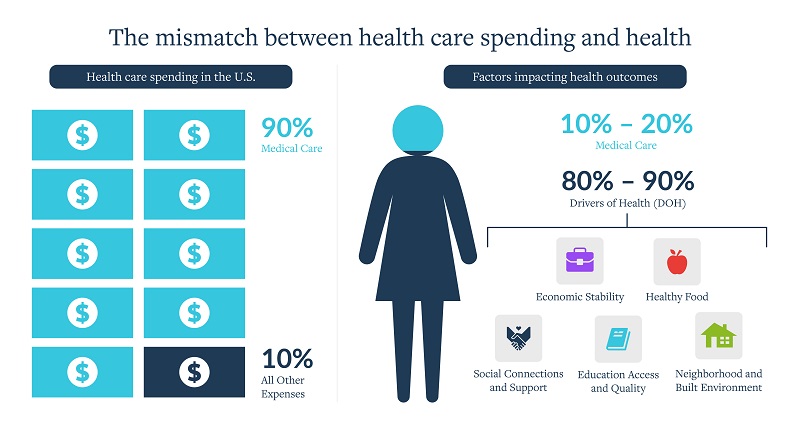
This isn’t really new news. We knew social connections were critical long before the Surgeon General’s proclamation. In fact, research on the drivers of health (DOH), also known as social determinants of health, highlights that DOH are responsible for up to 80-90% of our health outcomes. And by both the CDC’s and WHO’s definitions, social connections are a key driver.
Yet, as a society, we are increasingly disconnected. In a recent Meta-Gallup survey, nearly 25% of adults across 142 countries reported feeling “very lonely” or “fairly lonely.” That’s one in four adults.
Notably, the most lonely cohort included those between 19-29 years old, and the least lonely were those over 65. What has changed in our society to exacerbate disconnections and raise loneliness—and its associated health impacts—to dangerously high levels?
Many things about society and interaction have changed in the past 15 years, but the introduction of smartphones significantly fueled the loneliness epidemic and associated negative health outcomes. As detailed in this Atlantic article from 2017, and reaffirmed by Jonathan Haidt’s latest research, smartphones were not a smart bet for our mental health. They hurt children, especially girls, but the harm isn’t limited to children. It’s pervasive across society.

Image source: The Atlantic
Haidt points out in his research that carrying smartphones, and the consistent access to the internet and social media they provided, altered daily experiences and developmental pathways for adolescents. It changed the way they made friends, dated, slept, exercised, thought about politics, and interacted with their families. My colleague Julia Freeland Fisher recently argued that because of the incredible influence of smartphones and the now-ubiquitous emergence of AI into daily life, “prioritizing prosocial behavior, investing in deeper family engagement, and leaning into the power of real-world” experiences are no longer nice-to-haves. Instead, these are must-haves if we seek to ensure healthy human development and behavior.
While less relevant for developmental pathways, smartphones also changed social factors for adults. Smartphones enabled adults to date, make friends, interact, engage with politics, etc., in ways that weren’t previously possible. As a result, we have an increased need for prosocial countermeasures for people of all ages.
Disruptive Innovations and their impact on health
As someone who studies the impact that Disruptive Innovations have on our health care industry, and thus on our collective health, I couldn’t shake the eerie feeling and a question Haidt’s latest research left me to grapple with: When it comes to worsening loneliness, are we on the brink of the second wave?
Is there another Disruptive Innovation—generative AI and the ways it is being deployed in potentially disruptive business models—that is poised to have equally bad, or worse, impacts on our health? In short, I’m wondering how the growing role of AI in our lives will exacerbate our loneliness and the associated negative health outcomes.
It might start as a small switch. It could be something as seemingly harmless as asking ChatGPT to answer a question instead of turning to a colleague, spouse, friend, or even thinking for ourselves. But these small choices all have impacts. They create habits, and we know those are hard to change.
Trade-offs associated with using generative AI in health care
Generative AI—artificial intelligence capable of generating text, images, videos, or other data using generative models (learning the patterns and structure of input training data and then generating new data that has similar characteristics), often in response to prompts—has been touted as a miracle solution to many of the problems we face in the industry today, especially in our labor-constrained environment. For example, generative AI can help with the loneliness crisis for our growing number of aging elders (though I question if it truly “helps”); it can alleviate doctors’ need to chart for hours after shifts have ended; it can even speed up research analysis for drug discovery; and it can do much, much more.
As with all innovations, there will be trade-offs. Each time we trade an interaction with AI for a speedy response, we trade-off something else with it. We lose the opportunity to connect with another person.
We aren’t just trading off a conversation with a physician for a conversation with a chatbot. We are trading human connection for human disconnection. And the compounded cost of these trade-offs over time has a negative impact on our health.
So, what I hope we will think about as an industry is, “Which trade-offs are we willing to make?” To tackle this question, it would help us to ask the following:
- How are we measuring “success” as we implement generative AI in the industry?
- What are the unexpected externalities of leveraging generative AI in health care encounters?
- As an industry, do we truly value the drivers of health? If so, can we afford the cost of overemphasizing speed, efficiency, and cost-effectiveness, at the expense of human connection?
I don’t have all the questions, and I certainly don’t have all the answers. But we are at a societal inflection point. One where I just can’t shake the feeling and question Haidt’s research left me to address. As I grapple with these questions in my research, Winston Churchill’s 1948 quote is ringing in my ears, “Those that fail to learn from history are doomed to repeat it.”
We didn’t know what we didn’t know when smartphones became ubiquitous. Now we know.
So, I’ll leave you with this question: Will we make different trade-offs this time?
I asked ChatGPT. Its response was inconclusive…
