
It’s officially predictions season! I’ll start with my usual emphasis: What makes this piece worth reading is the combination of my experience in health care and the application of the theories of Disruptive Innovation. These theories help us see around corners, even if—as many could argue is the case in health care today—it’s a corner we’d rather not see around at all.
For a reminder of theory’s power, check out last year’s health care predictions. In my assessment of our 2025 forecast, theory got an A on the test. Related to the last prediction I outlined for 2025, I encourage you to check out Science to People. It’s a great example of how—even in the face of misinformation’s disruption of expertise—public health, health care, and scientific leaders are responding in powerful ways.
This year, I’m also emphasizing that I didn’t use AI to write or edit this. I did rely on my impeccable human editor, who not only makes my writing better, but is also a lovely person. Are there humans in your life you prefer to rely on more than AI? If so, you’re living into one of my predictions for 2026.
In this piece, I’m focusing on three predictions for health and health care in 2026 and beyond:
- Healthspan breakthroughs will come from relationships, not algorithms
- Pressure to change health insurance will increase, but progress will be slow
- AI won’t transform health care delivery business models…yet
There may be many disagreements with this last prediction, so please share your thoughts. Let’s dive into it.
1. Healthspan breakthroughs will come from relationships, not algorithms
In the years since the COVID-19 pandemic, we’ve seen social health and social connection rise in popularity. If you aren’t familiar with it, social health is the component of overall health that stems from quality human connections. Conveying its position in the zeitgeist, Google Trends provides a nice graph of how searches for “social health” have skyrocketed in recent years.
In health care, entities like Social Prescribing USA, the prior Surgeon General’s work (here, here, and here), and thought leaders like Kasley Killam are bringing overdue attention to this underemphasised driver of health. And as social health becomes both more popular in the zeitgeist and more discussed in health care environments, 2026 will further emphasize its importance.
Alleviating loneliness is top of mind for many, especially as more adults are grappling with it. A recent survey from AARP highlighted that 40% of adults 45 and older now report being lonely, up from 35% in 2010 and 2018. As a result, many have desired progress (one key component of a Job to Be Done) that includes “help me feel less lonely.” We also know loneliness raises our risk for poor physical and mental health outcomes.
Yet, while extensive research highlights the role of drivers of health (a.k.a. social determinants of health) in improving our health outcomes, and these drivers have received increasing attention in health care over the past decade, we’re still lagging in the specific focus we place on social health and the associated social connections and support. As a critical driver of health (see the right-hand side of the graphic below), this is to our detriment.
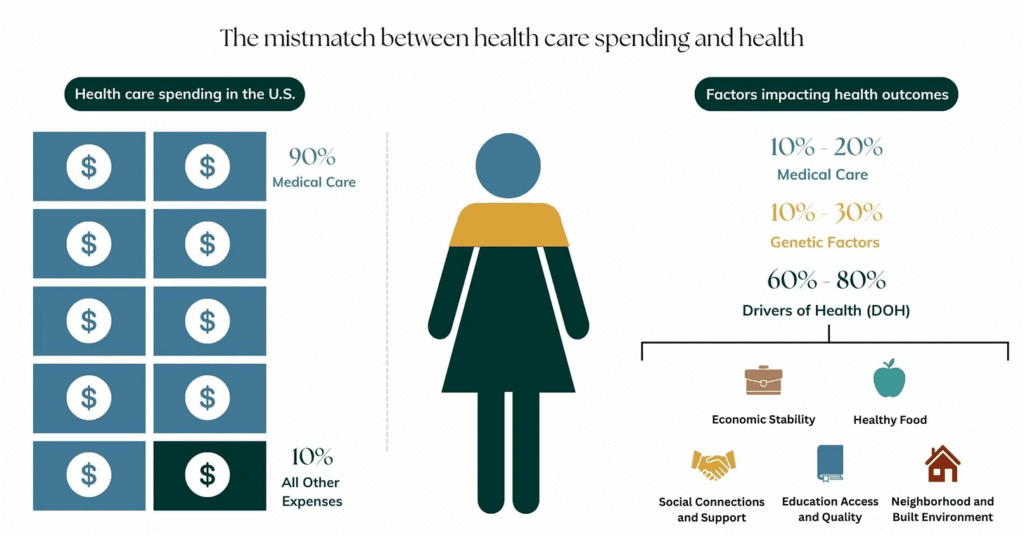
What gets measured gets managed. Social health deserves the same level of attention as blood pressure checks, cholesterol labs, and bone density scans. I hope 2026 will bring such a measure into the mainstream (though given the time required for such a change, I don’t “predict” it will occur). Longitudinal relationship data show that the impact of deep, meaningful human connections on our health is extremely beneficial. And in today’s AI-everything environment, it’s easy to downplay the benefit of human connection and believe that AI can solve all of our loneliness problems. But that would be to our detriment (see also my colleague Julia Freeland Fisher’s work here).
Both new and well-established research support this assertion, and most humans intuitively know this to be true. 2025 saw many studies show that AI isn’t all positive for health outcomes, especially for young people. Additionally, as generative AI falls from the peak of the Hype Cycle, we’re realizing that AI isn’t the ideal replacement for human relationships that many think it can be. (Even Michael Burry, of The Big Short fame, predicts OpenAI might be the next Netscape.)
In 2026, human connection won’t just gain popularity in health and health care, but, as The Future Laboratory predicts, it will pervade various industries, including sport, hospitality, and more. People long for deep, meaningful human relationships, and in 2026, we’ll see this desire pervade health and health care culture. In a year with potentially dark overtones, this has the potential to be a shining light if individuals and policymakers work intentionally to create both prosocial environments and prosocial AI tech.
2. Pressure to change health insurance will increase, but progress will be slow
Like many of you, I read the Keckley Report weekly to hear industry oracle Paul Keckley dissect what’s just occurred in the industry and what’s likely over the horizon. Throughout 2025, and even in 2024, he has repeated the theme that we are at an inflection point in health care: it’s too expensive, and the public backlash can no longer be ignored. He also rightly notes that while outsiders desperately want change, insiders resist it. This is exactly the behavior that Christensen’s business model theory predicts.
Keckley is absolutely correct that we’ve reached an inflection point. But while there’s demand for change, and few would argue that change is unnecessary, it won’t be fast. Why? Because of how business models work.
A business model consists of four interlocking components that, when taken together, create and deliver value (see image below). In an organization’s early days, all components of the business model are flexible. To survive, organizations pivot their value propositions and adjust their resources and processes until they identify how to generate the revenue they need to survive. Once this is determined, business model components become increasingly interdependent and resistant to change, especially in successful organizations. The ways in which the four components reinforce one another make the business model highly interconnected and more challenging to alter over time.
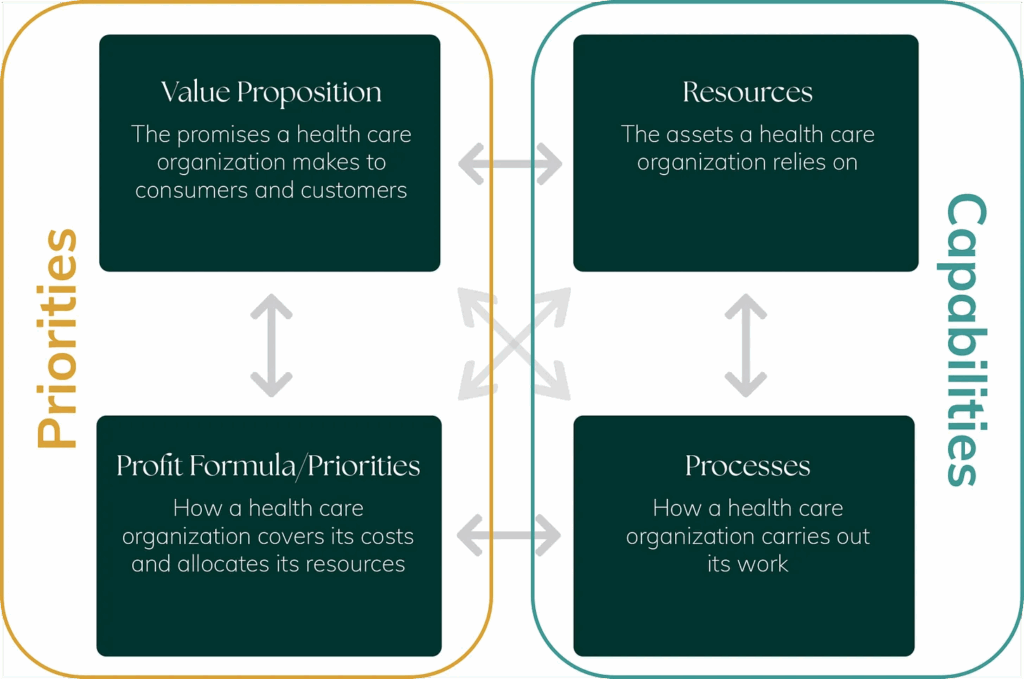
This is why innovations often come from new entities. It’s more effective to innovate in a business model that hasn’t solidified to deliver on a purpose that conflicts with the innovation. Business model innovation can seed transformation, but innovative business models need a new value network—the ecosystem of suppliers, partners, distributors, customers, other institutions, and regulations a company interfaces with to establish and maintain its model—to scale. Without scale, the industry can’t transform.
Business models determine an organization’s capabilities and its priorities, but a value network determines the resources an organization has access to, the rules it must follow, and the permissions it needs to operate. It also includes external entities with varying degrees of power to shape the organization’s priorities through resource dependence, regulation, and governance.
So, yes, there is both societal and political pressure for change, but due to entrenched business models and the overall complexity of health care, change will be slow. Slow doesn’t mean nonexistent, but we shouldn’t expect a fundamental overhaul or a resulting cost decline in health insurance this year.
However, I’ve included a few promising ideas and approaches we should all be watching as innovators seek to create a groundswell necessary for sustainable improvement:
- Life for Health: A proposal for a new system to solve chronic disease using life insurance. Focusing initially on metabolic issues like obesity and diabetes, it creates long-term alignment between insurers and individuals to reverse disease, maintain better health, and prevent recurrence or onset. Everyone, over time, shares in the value created by less disease.
- Fund The Patient: Advocacy for a new approach that gives “doctors, patients, and health care policy experts more choice, more control, and proper funding” so people, with their doctors, can make the best health care decisions.
- ICHRA: As I’ve written about before, ICHRA isn’t a cure-all to our health care woes, but as Christina Farr has written about more extensively than anyone, it does show promise in an environment where employers are eager to spend less, and employees are eager to both save more and not have their insurance tied to their employment.
Business model change is required to dramatically improve health insurance, and while there is both cultural and political impetus to spur it, it won’t happen quickly. Progress in 2026 will be slow.
3. AI won’t transform health care delivery business models…yet
Lastly, I do have an AI prediction. First, let’s level-set on what AI is and isn’t. AI isn’t a disruptive innovation. It’s a resource. And resources aren’t disruptive in and of themselves. Business models disrupt business models. And to be successful, innovative business models must be surrounded by a supportive value network.
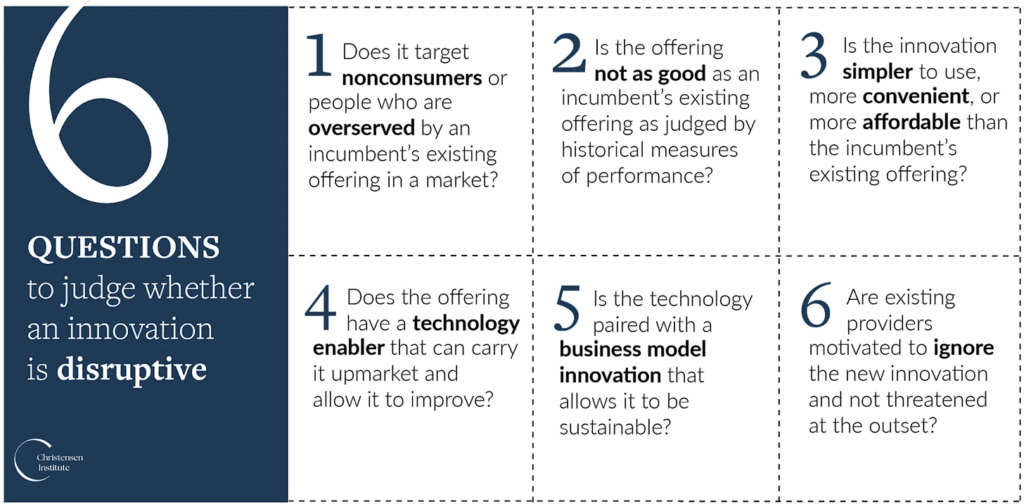
If AI is going to “disrupt health care,” we need to specify which business model powered by AI poses a disruptive threat, and what it’s disrupting. That’s important because disruption is relative. (See below for our 6-question test to assess disruptive potential.)
This year, my most-read piece on AI was “OpenEvidence: Disruptive or not? Plus, why it matters.” In it, I conclude that while OpenEvidence is clearly changing the process of care delivery, it doesn’t pose a disruptive threat to UpToDate, at least not in its current form. However, that doesn’t mean it won’t change the game. It already has. It also doesn’t mean it won’t outcompete UpToDate or other alternatives. Even if they aren’t disruptive innovations, new entrants can succeed in the market because they serve a Job to Be Done better than the competition. Uber is an excellent example of this.
What does this phenomenon have to do with other health care AI solutions? AI has been most effectively deployed in health care as an RCM solution, a scribe solution, and a clinical decision support tool. Many of these new AI-driven business models succeed because they operate within existing business models and value networks.
But they haven’t yet disrupted traditional provider business models (i.e., hospitals and clinics). They have made care delivery more efficient, improved the provider experience, and in some ways improved care for existing customers (a sustaining innovation). They haven’t fundamentally changed the value proposition of provider organizations or how providers get paid at scale, which means the business model (see above) hasn’t been transformed. While they might spur such changes in the long run, they won’t accomplish this feat in 2026. Disruption and business model transformation are processes that unfold over time, often over decades.
That doesn’t mean we should lose hope. It means we should pay close attention. Shining a light on AI’s potential to ignite transformative change in provider business models, I was excited to read a recent analysis by Blake Madden about AI-enabled primary care at Ochsner. The investment seeks to reduce the burden placed on a dwindling number of primary care providers in a state with worse health outcomes and higher disease burdens than much of the nation. It’s also a bet on CMS ultimately paying for outcomes, which is increasingly likely with the recent launch of CMMI’s ACCESS Model. For a vision of the future, check out Blake’s analysis.
AI-driven models like Oschner’s primary care pilot have the opportunity to transform health care because they offer a different value proposition, leverage different capabilities to deliver it, and rely on a different profit formula than traditional health care models. And, such transformative change takes time.
What would you add? I’d love to hear what you think theory got right and what we missed. I read all of my emails and look forward to your input.
